Hong-Xia Cui ![]() ,
En-Liang Wu
,
En-Liang Wu
For correspondence:- Hong-Xia Cui Email: hxiacui@163.com
Received: 10 May 2016 Accepted: 10 September 2016 Published: 31 October 2016
Citation: Cui H, Wu E. Effect of levocarnitine/iron saccharate combination on renal anaemia and oxidative stress in patients undergoing haemodialysis. Trop J Pharm Res 2016; 15(10):2269-2274 doi: 10.4314/tjpr.v15i10.28
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To investigate the effect of a combination of levocarnitine and iron saccharate on the treatment of renal anaemia and oxidative stress in patients undergoing haemodialysis.
Methods: A total of 156 patients with renal anaemia were divided randomly into control (78 cases) and test groups (78 cases). Patients in the control group were treated with erythropoietin (EPO), iron saccharate, and conventional symptomatic treatment, while patients in the test group were treated with levocarnitine additionally. Anaemia indices, oxidative stress indices, response rate, and EPO dose were compared.
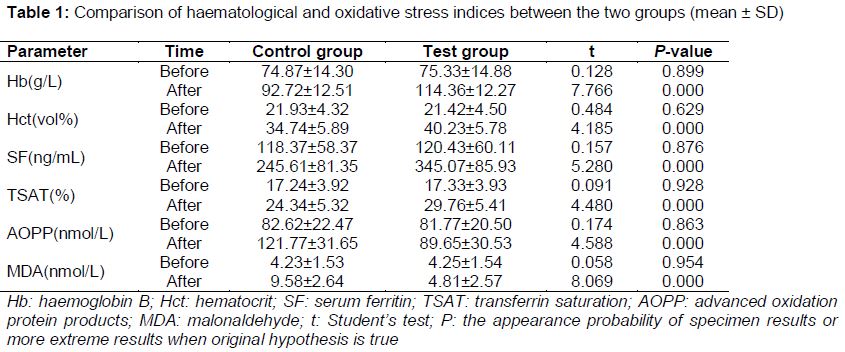
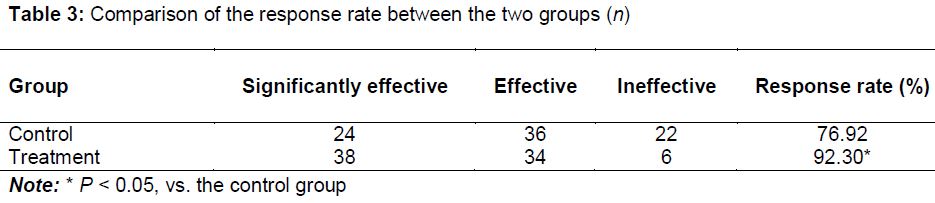
Results: At week 28, the levels of hemoglobin b (Hb), hematocrit (Hct), serum ferritin (SF), and transferrin saturation (TSAT) in the test group were 92.72 ± 12.51 g/L, 34.74 ± 5.89 vol %, 245.61 ± 81.35 ng/mL, and 24.34 ± 5.32 %, respectively, which were much lower than the levels in the test group (114.36 ± 12.27 g/L, 40.23 ± 5.78 vol %, 345.07 ± 85.93 ng/mL, and 29.76 ± 5.41 %, respectively; p < 0.05). The levels of advanced oxidation protein products (AOPP) and malonaldehyde (MDA) in the test group were much higher than those of the control group (121.77 ± 31.65 nmol/L vs 89.65 ± 30.53 nmol/L; 9.58 ± 2.64 nmol/L vs 4.81 ± 2.57 nmol/L, respectively (p < 0.05). EPO was maintained at a high dose from the beginning of treatment to week 28 in the control group, whereas in the test group, EPO dose was reduced gradually. The response rate in the test group was higher than that in the control group (92.30 % vs 76.90 %; p < 0.05).
Conclusion: Levocarnitine/iron saccharate combination had a significant positive effect on the treatment of renal anaemia. It effectively relieved oxidative stress reactions and reduced the dose of EPO required.
Introduction
Renal anaemia, a commonly observed complication in patients with chronic renal failure during the terminal stage, occurs when the glomerular filtration rate (GFR) is reduced by over 50 % [1,2]. Renal anaemia can induce abnormalities in multiple physiological functions, as well as cardiovascular and cerebrovascular diseases, thereby influencing the quality of life of patients with chronic kidney disease and lowering survival rates. Fortunately, erythropoietin (EPO) can relieve anaemic symptom in patients with chronic renal failure [3]. However, some patients with renal anaemia who undergo haemodialysis treatment respond poorly or not at all to EPO because of iron deficiency, chronic infection, and malnutrition [4,5]. Thus, supplementing with iron saccharate is usually regarded as an adjuvant therapy. However, researchers [6,7] have found that iron saccharate can induce an increase in oxidative stress reactions and the occurrence of cardiovascular and cerebrovascular events. Thus, antioxidant interventions are also important in patients undergoing haemodialysis.
Levocarnitine, also called L-carnitine [8], is an amino acid that is extensively distributed in body tissues and is used for the treatment of several chronic renal failure - associated complications in patients who undergo long-term haemodialysis and develop secondary carnitine deficiency. Levocarnitine can significantly relieve malnutrition and antioxidation, allowing the EPO dose to be lowered, thus reducing the economic stress on patients. This study evaluate the curative effect of iron saccharate combined with levocarnitine in renal anaemia and oxidative stress. To this end, the clinical effects of iron saccharate alone and iron saccharate in combination with levocarnitine were compared in treating chronic renal anaemia in patients undergoing haemodialysis were compared.
Methods
Study setting, design and patient characteristics
A total of 156 patients with renal anaemia who underwent haemodialysis between March 2011 and June 2014 at Binzhou People’s Hospital, Shandong, China, were selected randomly. The study was approved by the Medical Ethics Committee of Binzhou People’s Hospital (approval number: CHX20150518BZ), and conformed to the principles of the Declaration of Helsinki [9]. Those with stable disease conditions for at least 1 month, who underwent haemodialysis 2 or 3 times per week, who had a haemoglobin (Hb) level < 90 g/L, a serum ferritin (SF) level < 200 ng/mL, or a transferrin saturation (TSAT) < 20 %, and who signed the informed consent form (themselves or a family member) were included. Those who suffered from other severe complications or endocrine diseases or who had been treated with chalybeate were excluded.
The patients were divided into control (n = 78) and test (n = 78) groups using the random number table method. In the test group, there were 40 males and 38 females, with ages ranging from 34 to 66 years (average 49.46 ± 10.13) and a haemodialysis period of 17.6 – 43.3 months. In the control group, there were 42 males and 36 females, with ages ranging from 35 to 67 years (average 49.57 ± 9.97) and a haemodialysis period of 18.2 – 43.6 months. Age, gender, and duration of haemodialysis were not significantly different between the groups (p > 0.05); thus, the results were comparable.
Treatment
Based on maintenance haemodialysis, patients in the control group were treated with EPO and iron saccharate. EPO (Chengdu Diao Jiuhong Pharmaceutical Co., Ltd., Sichuang, China; batch No.: S20020060) at doses 150 – 200 U/kg was injected subcutaneously. Hb levels were measured every 4 weeks. If the Hb level increased to < 10 g/L, then the EPO dose was increased by 25 U/kg each time; if the Hb level exceeded the normal value, then the EPO dose was decreased by 25 U/kg each time. Moreover, 100 mg iron saccharate (Nanjing Hengsheng Pharmaceutical Co., Ltd., Jiangsu, China; batch no. H20113004) were injected through the vein end of the dialysis tube after each haemodialysis session. In the treatment group, the same procedure as that in the control group was followed, but the patients were additionally injected intravenously with 1.0 g levocarnitine (batch no. H20050443; Haiyue Pharmaceutical Co., Ltd, Jilin, China) and 20 mL normal saline after haemodialysis. Patients in both groups were treated for 28 weeks.
Determination of parameters
Levels of Hb, haematocrit (Hct), TSAT, advanced oxidation protein products (AOPP), and malonaldehyde (MDA) before treatment and after 28 weeks of treatment were compared. The maintenance doses of EPO in the groups were recorded at the beginning of treatment and at weeks 14 and 28. The curative effect was determined according to the changes in the anaemia and oxidative indices [10]. The treatment was considered significantly effective if the Hb level improved to at least 30 g/L, the level of Hct increased to at least 0.1 vol %, or Hb and Hct both recovered to normal levels, and the anaemia symptoms improved significantly during treatment. The treatment was considered effective if the level of Hb improved to at least 15 g/L or the Hct increased to at least 0.05 vol % and the anaemia symptoms were relieved by the end of treatment. The treatment was considered ineffective if the levels of Hb or Hct showed little to no change or the anaemia symptoms were aggravated. The formula for the overall response rate (R) is as in Eq 1.
R (%) = {(S + C)/T}100 ……………………… (1)
S is the number of significantly effective cases, C the number of effective cases and T the total number of cases.
Statistical analysis
The SPSS software (ver. 19.0) was used for statistical analysis. Data expressed as mean ± standard deviation (SD), were analysed using the Student’s test. Numerical data were compared using the χ2 test. P values < 0.05 were considered to indicate statistically significant differences.
Results
Haematological and oxidative stress indices
Levels of Hb, Hct, SF, TSAT, AOPP, and MDA in the two groups showed no statistically significant difference before treatment (all p > 0.05). After 28 weeks of treatment, the levels of Hb, Hct, SF, and TSAT were significantly higher in the test group than the control group (p < 0.05), whereas the levels of AOPP and MDA were lower in the test group than in the control group (p < 0.05; ).
Comparison of EPO doses between the two groups
Throughout the treatment period, the required EPO dose in the control group remained relatively high, whereas the EPO dose in the test group was reduced gradually. At week 28, the EPO dose in the test group was significantly lower than that in the control group ().
Comparison of the curative effect between the two groups
The results suggested that the overall response rate in the test group was significantly higher than that in the control group 24 h after treatment (p < 0.05; ).
Discussion
Renal anaemia is typically induced by chronic renal failure, caused by multiple organic renal diseases. The internal and external secretory functions of the kidney weaken or fail completely when chronic renal failure occurs. The pathogenesis of renal anaemia is complex. Its clinical manifestations are often masked by primary renal diseases, especially in the initial stages.
With the extensive application of renal dialysis, patients with chronic renal failure now tend to have longer survival periods; however, the number of cases of chronic renal anaemia is also increasing [11]. A study [12] suggested that 26.50 % and 95.80 % of 110 patients with chronic renal failure developed anaemia during the renal insufficiency period and the uraemia period, respectively. Most patients undergoing maintenance haemodialysis will likely develop chronic renal anaemia, and anaemia can severely influence treatment efficacy and quality of life. Therefore, there is an urgent need to treat chronic renal anaemia in patients undergoing maintenance haemodialysis.
According to a previous study [13], EPO deficiency is the leading cause of chronic renal anaemia. Consequently, treating renal anaemia with EPO has been promoted in the early stages of the disease, and EPO can correct anaemia symptoms in most patients. However, recent clinical investigations suggest that about 10 % of patients with chronic renal anaemia show a poor response to EPO.
A clinical study [14] showed that levels of Hb and Hct may fail to reach normal values after treatment with EPO. The main reason is that iron deficiency greatly influences the curative effect of EPO treatment. Indeed, half of haemodialysis patients undergoing EPO treatment experience a poor curative effect due to iron deficiency. Repeated blood collection, residual blood in the dialyzer or pipeline, and the application of high-dose EPO can all result in iron deficiency. Moreover, iron in the storage pool may not be released in a timely manner, leading to a functional iron deficiency and a microinflammatory state [15]. As a result, chalybeate is usually given to renal anaemia patients undergoing haemodialysis during EPO treatment.
Iron saccharate is an important drug used for iron supplementation. Sucrose molecules that surround Fe(OH)3, the core of iron saccharate, prevent its elimination by the kidney. However, studies [16,17] have suggested that iron saccharate can result in increased oxidative stress reactions, although it is considered safe and has a definite effect in treating renal anaemia. Oxidative stress refers to the release of a large number of oxygen radicals, caused by respiratory burst, which occurs when reduced coenzyme II on the membrane of leukocytes is activated.
Levocarnitine, also called L-carnitine, is an amino acid that is extensively distributed in the body tissues and is necessary for the metabolism of fatty acids [18]. It has been shown that levocarnitine can promote the synthesis of albumins, significantly improve the stability of the erythrocyte membrane, increase Hct, and transport long-chain fatty acids into the body [19]. Patients undergoing maintenance haemodialysis tend to have insufficient levocarnitine, due to a lack of levocarnitine before treatment, severe loss during treatment, and the consumption of levocarnitine during treatment. Levocarnitine deficiency can affect metabolism, increase the fragility of normal red blood cells, and shorten the life of these cells [20].
This study found that the levels of two major oxidative stress markers, AOPP and MDA, were increased significantly in both groups before treatment, suggesting the presence of oxidative stress. After 28 weeks of treatment, the levels of AOPP and MDA increased markedly in both groups, indicating that iron saccharate resulted in a further increase in oxidative stress. However, the increases in the levels of AOPP and MDA were less in the test group than the control group at week 28 (p < 0.05), suggesting that levocarnitine had an antioxidant effect that could relieve the oxidative stress induced by iron saccharate.
It was also found that the levels of Hb, Hct, SF, and TAST of the patients were higher in the test group than the control group at week 28. The dose of EPO in the test group, which was decreased gradually, was lower than that in the control group at week 28. This suggested that levocarnitine could improve the curative effect of EPO, and that the combined use could significantly relieve the anaemia symptoms of patients undergoing haemodialysis and lower the dose of EPO. The mechanism of action might be because levocarnitine promotes the absorption of EPO by acting on erythroid progenitor cells [21].
Study limitations
No adverse reaction was observed in the research subjects, which differs from the findings of other studies. It is considered that this was associated with the small sample size. Therefore, a study with a larger sample size is required to evaluate the safety of levocarnitine in combination with iron saccharate in treating renal anaemia.
Conclusion
Levocarnitine combined with iron saccharate has a positive therapeutic effect on renal anaemia in patients undergoing haemodialysis. The therapy significantly improves anaemia and oxidative stress indices and patient quality of life and reduces the damage caused by oxidative stress. However, the indications and conditions for administering the drugs must be established first, particularly in elderly patients whose physical and organ functions are weaker.
Declarations
Acknowledgement
References
Archives


News Updates